Authors
Cole Maguire & Katherine Motovilov

Close
Sponsored by Kathleen C. Moore Foundation & Novartis

7 Jun 2026 | ~05:18 Engagement Time
Uhthoff’s Phenomenon is a well-known feature of multiple sclerosis (MS) in which patients experience a temporary worsening of their MS-related, neurological symptoms when their body temperature increases during every-day conditions/activities – such as hot weather, baths, saunas, exercise, or fevers. In fact, this temperature-sensitivity is so common that having patients sit in a hot water bath used to be part of the MS diagnostic procedure! Patients often report heat-sensitivity as having a significant, negative impact on their quality of life, especially those living in warm climates. Thus, many MS patients often want to know whether these temporary flares may take a greater toll on their health and if it is safe to be exposed to hot weather, exercise, or partake in activities like saunas. Here, we give an overview on what is currently known about Uhthoff’s Phenomenon and tackle some of the common questions MS patients experiencing Uhthoff’s may have.
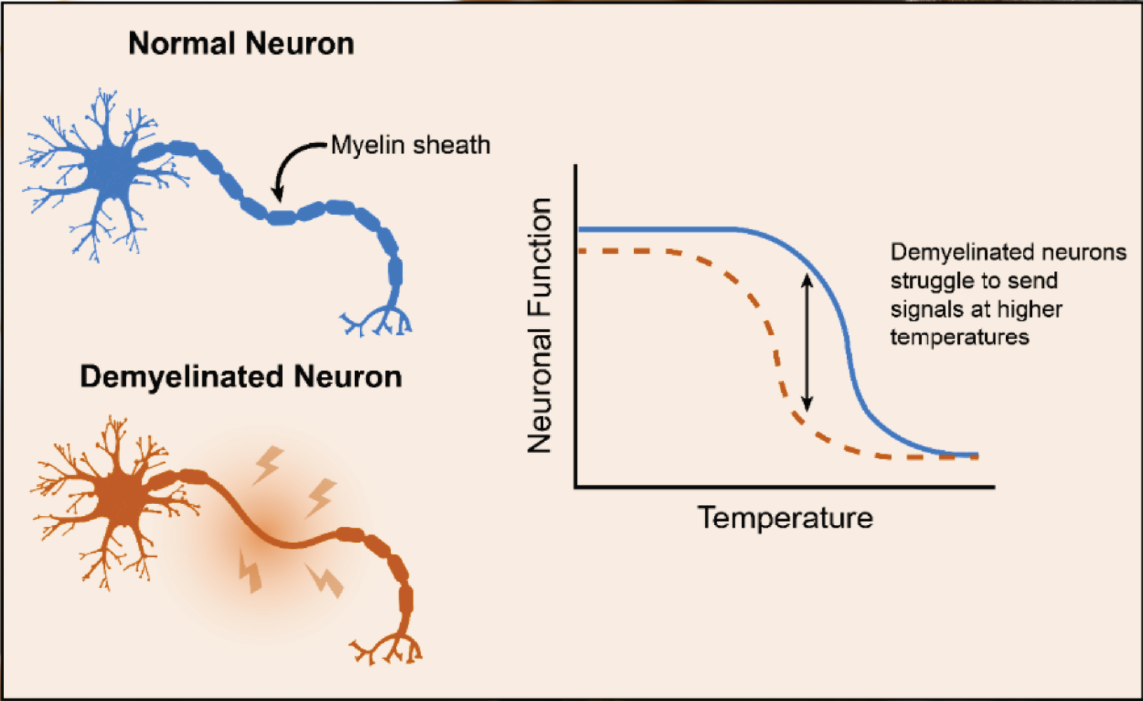
The mechanisms underlying Uhthoff’s Phenomenon are not well-understood. While several factors have been proposed to contribute, the most widely accepted theory is ‘central conduction block’. Central conduction block is an interruption in electrical signaling of the central nervous system which manifests as delays or interruptions in neuronal communication. These neuronal disturbances can manifest as physical symptoms including weakness, trouble with thinking, attention, concentration, and memory. While all individuals, including those without MS, have a temperature limit at which their neurons will struggle to conduct electrical signal, the central conduction block theory proposes this temperature limit is lowered in patients experiencing demyelination from MS.
Demyelination is an event in which the myelin sheath (a layer of insulation which coats the neuron, similar to rubber on a copper wire) is broken down and is the fundamental disease process underlying MS. The destruction of neuronal insulation, itself, causes difficulties in neuronal signaling, which manifests in traditional MS symptoms. Thus, in individuals with MS, relatively small elevations in body temperature, such as those occurring with exercise, in hot weather, or during a fever, become sufficient to disrupt the spine and brain’s electrical signaling. Of note, other theories for the cause of Uhthoff’s phenomenon have also been proposed, which may include signals from heat-responsive proteins (known as heat-shock proteins), effects of calcium levels circulating in the blood, and blocks in intracellular channels which pass charged particles (critical for electrical signals passing through the central nervous system).
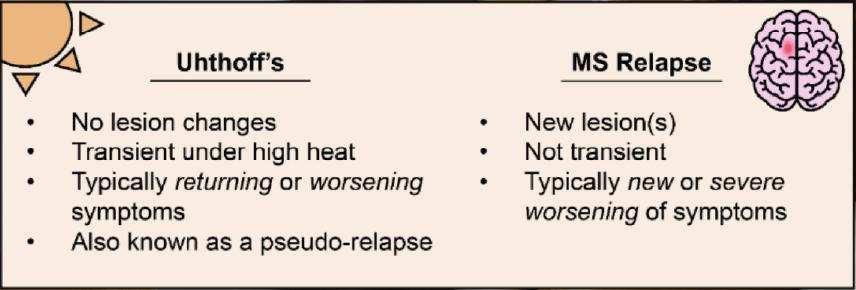
Uhthoff’s phenomenon is often referred to as a “pseudo-relapse”. Currently, there is no evidence that demonstrates any correlation between the experience of temperature-induced worsening of symptoms and the formation of new lesions or initiation of a true clinical relapse in MS. This means that while the experience may be uncomfortable and disruptive, individuals with MS do not need to be concerned for your disease progression when you experience Uhthoff’s phenomenon. However, this distinction may sometimes be challenging to interpret, making it difficult to know when patients should seek medical attention. Key differentiating factors between symptom flares from Uhthoff’s and true MS relapses can include timing, symptom profile, and duration of flare. Symptom exacerbation linked to Uhthoff’s phenomenon will always be linked to elevations in body temperature, should resolve within approximately a day, and should not typically bring new symptoms. Notably, while Uhthoff’s can be triggered by fever following illness, infections are known to sometimes correlate with relapse occurrence and should be monitored carefully (Correale et al., 2006).
Uhthoff’s Phenomenon was first described in 1890, giving it a strong foothold to influence treatment strategy in MS for over 100 years. Originally, the existence of heat-sensitivity in patients led to a conservative approach by clinicians and physiotherapists, limiting the use of physical activity or any form of heat exposure in MS (Opara et al., 2016). However, multiple studies now exist which highlight the benefits of aerobic exercise for people with MS, with improvements in physical fitness helping to prevent disability progression, improving fatigue, and boosting quality of life (Kileff & Ashburn, 2005; Lord et al., 1998; Pariser et al., 2006; Petajan et al., 1996). Therefore, it is now generally recommended for individuals with MS to engage in physical activity and exercise when safe and feasible, including strength training and light cardio.
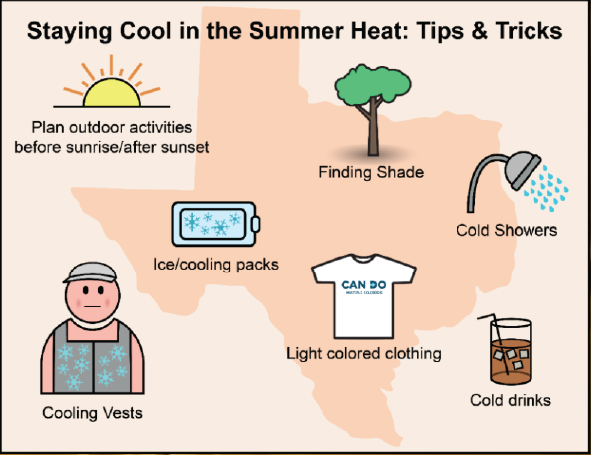
Many patients with MS living in Texas or areas with similar climates have difficulties in navigating daily activities during the summer months due to their experience with Uhthoff’s Phenomenon. While heat-induced symptom worsening is typically thought of as a transient event, recent work from our lab demonstrates that some individuals have persistence of their Uhthoff’s-related symptoms for up to 24 hours or even longer after heat-exposure (Katherine Motovilov et al., 2025). This suggests that the most effective strategy for patients is to prevent elevations in body temperature to the best of their ability, by strategically timing outdoor activities (taking advantage of cooler temperatures at sunrise/sunset), finding shade, and using active cooling measures. Cooling measures can include taking cold showers, drinking cold beverages, wearing loose, light colored clothes, and applying ice packs or other targeted cooling devices to areas like the back of the neck or under the armpits. Recently, cooling garments such as cooling vests or cooling hats have also become a common tool for patients with MS who are exposed to hot temperatures for prolonged periods of time. Notably, the use of cooling vests has additional benefits including reducing fatigue and improving motor function/vision in some patients, making them a potentially worthwhile investment (Panginikkod et al., 2026).
Some reports have also suggested that the oral medication 4-aminopyridine (dalfampridine, Ampyra) may reduce the worsening of visual impairment associated with heat-exposure in some patients with MS by making it easier for electrical signals to be propagated in the central nervous system (van Diemen et al., 1992). While dalfampridine has been approved by the Food and Drug Administration (FDA) to improve walking capacity in patients with MS, its benefits in Uhthoff’s phenomenon, specifically, remain unclear.
While the precise mechanisms underlying Uhthoff’s Phenomenon remain uncertain, it is clear that many patients would benefit from an improved understanding of this condition and the development of new therapies for heat sensitivity in MS. In the meantime, stay cool and always contact your physician if you have any questions or concerns!
Correale, J., Fiol, M., & Gilmore, W. (2006). The risk of relapses in multiple sclerosis during systemic infections. Neurology, 67(4), 652–659. https://doi.org/10.1212/01.wnl.0000233834.09743.3b
Katherine Motovilov, Sam Bazzi, Cole Maguire, QingqingWang, Elizabeth Williams, Bryan Clements, Maisey Schuler, Max Weed, Christina Mihova, May Han, David Paydarfar, & Esther Melamed. (2025). Temperature sensitivity associates with indicators of disease progression in multiple sclerosis. 31(3), 167–167.
Kileff, J., & Ashburn, A. (2005). A pilot study of the effect of aerobic exercise on people with moderate disability multiple sclerosis. Clinical Rehabilitation, 19(2), 165–169. https://doi.org/10.1191/0269215505cr839oa
Lord, S. E., Wade, D. T., & Halligan, P. W. (1998). A comparison of two physiotherapy treatment approaches to improve walking in multiple sclerosis: A pilot randomized controlled study. Clinical Rehabilitation, 12(6), 477–486. https://doi.org/10.1191/026921598675863454
Opara, J. A., Brola, W., Wylegala, A. A., & Wylegala, E. (2016). Uhthoff`s phenomenon 125 years later—What do we know today? Journal of Medicine and Life, 9(1), 101–105.
Panginikkod, S., Rayi, A., Rocha Cabrero, F., & Rukmangadachar, L. A. (2026). Uhthoff Phenomenon. In StatPearls. StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK470244/
Pariser, G., Madras, D., & Weiss, E. (2006). Outcomes of an aquatic exercise program including aerobic capacity, lactate threshold, and fatigue in two individuals with multiple sclerosis. Journal of Neurologic Physical Therapy: JNPT, 30(2), 82–90. https://doi.org/10.1097/01.npt.0000282572.63297.3d
Petajan, J. H., Gappmaier, E., White, A. T., Spencer, M. K., Mino, L., & Hicks, R. W. (1996). Impact of aerobic training on fitness and quality of life in multiple sclerosis. Annals of Neurology, 39(4), 432–441. https://doi.org/10.1002/ana.410390405
van Diemen, H. A., van Dongen, M. M., Dammers, J. W., & Polman, C. H. (1992). Increased visual impairment after exercise (Uhthoff’s phenomenon) in multiple sclerosis: Therapeutic possibilities. European Neurology, 32(4), 231–234. https://doi.org/10.1159/000116830
Keep Learning...
But wait, there's more...
View All Related to Daily Life with MS: Symptoms




